
Peptides have become one of the most-discussed tools in weight-loss research — largely on the back of GLP-1 drugs that have posted the strongest results of any obesity intervention to date.
But "peptide" is doing a lot of work in that sentence. The five categories below are not equivalent. A couple of them have transformed obesity medicine. The others range from promising to preliminary. This guide breaks down what the evidence supports for each, and where the science is still thin.
Fat-loss peptides are short chains of amino acids — typically 2 to 50 — that act as signaling molecules influencing hunger, fat oxidation, glucose use, and energy output. The GLP-1 receptor agonists (semaglutide, tirzepatide) are the clinically validated leaders, with trial data showing roughly 15–22% average body-weight loss.
Everything else in this category — AOD-9604, the mitochondrial peptides, the GH secretagogues — sits well behind that on the evidence curve. Most are research compounds, not approved medications.
Fat-loss peptides are short chains of amino acids — typically 2 to 50 — that act as signaling molecules. These naturally occurring or synthetic compounds influence pathways tied to hunger, fat oxidation, glucose use, hormonal balance, and energy output. Unlike traditional weight-loss drugs that often work through a single mechanism, some peptides for weight loss can act on multiple pathways at once.
Peptides are smaller than proteins but larger than individual amino acids. They bind to specific receptors on cell surfaces, triggering cellular responses. In the context of weight loss, peptides may influence:
Not every peptide promotes fat loss. Some, like BPC-157, are studied for tissue repair and recovery instead. The compounds in this guide specifically target pathways involved in body composition, and have been studied in the context of weight management.
Peptides for weight loss operate through several distinct but often interconnected mechanisms. Understanding these clarifies why different peptides produce different results, and why individual responses vary so much.
Many weight-loss peptides, especially the GLP-1 agonists, mimic hormones that signal fullness to the brain. They bind receptors in the hypothalamus — the brain's hunger-control center — reducing appetite and caloric intake. That makes a calorie deficit easier to maintain.
Some peptides directly boost the breakdown of stored fat and mobilize fatty acids for energy. AOD-9604 is the example most often cited. It's designed to target adipose tissue and trigger the release of stored fat, without the growth-promoting effects of full growth hormone.
Mitochondrial peptides and certain growth-hormone secretagogues can influence metabolic rate by improving cellular energy production and resting energy output. The theory is that this helps the body use calories more efficiently, even at rest.
Improved insulin response lets the body process glucose more effectively, reducing fat storage and making stored fat easier to access.
Peptides that influence growth hormone, cortisol, and the sex hormones can indirectly affect body composition — helping preserve muscle during weight loss and reducing stress-related fat storage.
Below are the five categories with the most research attention. They differ widely in mechanism, and in how much human evidence sits behind them — which is exactly why lumping them together is a mistake. PrymaLab's peptides and weight loss guide covers the category in depth.
GLP-1 (Glucagon-Like Peptide-1) pathway peptides are the most extensively studied and clinically validated compounds for weight loss. They include FDA-approved drugs like semaglutide (Wegovy, Ozempic), liraglutide (Saxenda, Victoza), and tirzepatide (Zepbound, Mounjaro — which also activates GIP receptors).
The standouts:
How they work: they delay gastric emptying, suppress appetite signals to the brain, improve blood-sugar regulation, and reduce food cravings. These are the strongest results seen with any weight-loss intervention to date.
Considerations: prescription-only, requiring medical supervision. Common side effects include nausea, vomiting, and GI discomfort. They're most effective alongside diet and exercise, and both cost and insurance coverage vary. PrymaLab studies these compounds in its weight-loss & metabolic category and its tirzepatide guide.
Dual and triple agonists activate multiple receptors simultaneously, for potentially enhanced effects. Tirzepatide (GLP-1/GIP) is already approved. Newer compounds like retatrutide (GLP-1/GIP/glucagon) are in advanced trials.
The standouts:
The early data goes even higher. Phase 2 trials of retatrutide reported up to roughly 24% weight loss at 48 weeks — the highest of any obesity compound so far. The caveat: these are newer, and they have less long-term safety data behind them.
Considerations: newer, with evolving safety profiles. Prescription-only and medically supervised. Long-term effects are still under study.
AOD-9604 (Advanced Obesity Drug) is a modified fragment of human growth hormone — the C-terminal amino acids 177-191. It's engineered to keep HGH's fat-mobilizing properties while dropping its growth-promoting effects, which makes it a targeted lipolytic agent.
What the research describes: it stimulates lipolysis (fat breakdown), inhibits lipogenesis (new fat formation), and targets stubborn abdominal fat.
The evidence is mixed. A 2001 study in the Journal of Endocrinology reported weight loss in obese subjects, while others show more modest effects. Human clinical data is far less extensive than for the GLP-1 agonists, and AOD-9604 is not FDA-approved for weight loss.
On its regulatory status: AOD-9604 was placed on the FDA's Category 2 compounding list in 2023, citing significant safety concerns. It was removed from Category 2 in 2024 only because the nominator withdrew it — not because the FDA endorsed it. It remains a research compound.
Considerations: limited human data, variable results between individuals, and purity that varies between suppliers. Sourcing matters here more than almost anywhere else — see how to vet a supplier.
Mitochondrial peptides like MOTS-c and SS-31 (Elamipretide) are studied for improving cellular energy production and metabolic efficiency. They're not traditional "fat burners." The theory is that optimized mitochondrial function may indirectly support fat loss by improving overall metabolic health.
The compounds: MOTS-c (regulates metabolism), SS-31/Elamipretide (mitochondrial-targeted antioxidant), and Humanin (a mitochondrial peptide with metabolic effects). They're thought to improve mitochondrial efficiency, enhance fat oxidation, reduce oxidative stress, and support insulin sensitivity.
An honest note on the evidence: the research here is early. Animal studies show promising effects on metabolism and body composition, but human trials specifically for fat loss are limited. These are studied more for metabolic health and aging than for direct weight loss. Any effects are likely subtler than what you'd see from an appetite suppressant.
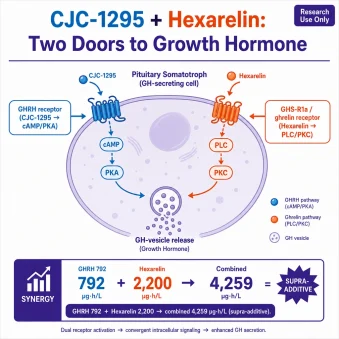
GH-releasing peptides that influence satiety and IGF-1 are the last approach in this list. Growth hormone secretagogues like CJC-1295 and ipamorelin are studied for stimulating the pituitary, and for their possible effects on body composition and appetite. Sermorelin belongs to the same group. Tesamorelin, a GHRH analog, is FDA-approved for HIV-associated lipodystrophy.
How they work: they stimulate natural GH release, influence satiety signals, support muscle preservation during weight loss, and may improve sleep quality — which itself affects metabolism.
The evidence: Tesamorelin has FDA approval specifically for reducing excess abdominal fat in HIV-positive patients, with trials showing significant visceral-fat reduction (Falutz et al., 2010). CJC-1295 and ipamorelin have less direct weight-loss evidence. They're widely studied for body composition and raising IGF-1, but their effects appear subtler than the GLP-1 agonists. See PrymaLab's Tesamorelin guide.
| Peptide Category | Primary Mechanism | Clinical Evidence | Availability | Regulatory Status |
|---|---|---|---|---|
| GLP-1 Agonists (Semaglutide, Tirzepatide) |
Appetite suppression, delayed gastric emptying | Strong | Widely available | FDA-approved for weight loss |
| Dual/Triple Agonists (Tirzepatide, Retatrutide) |
Multiple hormone pathways (GLP-1, GIP, Glucagon) | Strong/Emerging | Increasing | Tirzepatide approved; Retatrutide investigational |
| AOD-9604 | Lipolysis, fat mobilization | Moderate | Research compound | Not FDA-approved for weight loss |
| Mitochondrial Peptides (MOTS-c, SS-31) |
Metabolic optimization, energy production | Emerging | Research compound | Not FDA-approved for weight loss |
| GH-Releasing Peptides (CJC-1295, Ipamorelin, Tesamorelin) |
GH release, satiety signaling | Moderate | Research compound/prescription | Tesamorelin approved (HIV lipodystrophy); others investigational |
The evidence varies enormously across these categories. Understanding that spread is the whole point of this guide.
GLP-1 and dual agonists have the most robust evidence — multiple large-scale, randomized, double-blind, placebo-controlled trials with thousands of participants. That's the highest tier of medical evidence.
The other categories have far less human data behind them. Many of those studies are smaller, shorter, or built on animal models. The early results are promising. But more rigorous research is needed before anyone can claim long-term efficacy or safety.
Research consistently shows large individual variation in response. That's driven by genetics and metabolism, baseline body composition, age and hormonal status, dosage, and the diet and exercise around it.
Trial conditions are highly controlled and usually include full lifestyle support. Real-world results differ with adherence and support, so expectations should be grounded in individual circumstances.
Which compound (if any) is appropriate is a medical decision, made with a qualified provider.
In broad strokes: GLP-1 agonists fit those with significant weight to lose (15% of body weight or more), type 2 diabetes or insulin resistance, and appetite-control struggles — people who want an FDA-approved, extensively studied option.
Dual and triple agonists suit those who haven't reached their goals on a GLP-1 alone, and who want the most potent effects under close supervision.
AOD-9604 and the mitochondrial peptides are research-stage, studied for narrower or subtler use cases. The same goes for the GH-releasing peptides.
Only a licensed healthcare professional can determine whether any of these is appropriate for a specific situation. Self-prescribing is dangerous and highly discouraged.
Fat-loss peptides are not without risk. Understanding the potential side effects and contraindications is essential.
Common side effects vary by class, but often include:
For research compounds not approved by regulators, purity varies significantly between suppliers. Contaminated or mislabeled products pose real risks — which is why third-party testing and a Certificate of Analysis matter.
There's no simple yes or no. Safety depends on the specific compound, the dose, individual health, and — critically — medical supervision.
FDA-approved peptides (semaglutide, tirzepatide) have undergone extensive clinical testing and received FDA approval for weight management. Their safety has been assessed in thousands of patients. Used as prescribed and under supervision, they're considered relatively safe for appropriate candidates.
Research compounds haven't undergone the same evaluation. Long-term effects are less understood and quality control varies, so they carry more risk around purity and consistency.
Medical supervision isn't optional for prescription use. A provider evaluates history, screens contraindications, determines dosing, monitors for adverse effects, and ensures product quality.
Even for the approved peptides, data beyond 2–3 years is limited. For research compounds, it's largely unknown. That uncertainty should be part of any decision.
Peptides get the attention. But sustainable fat loss usually comes from stacking several proven strategies — which may be used alongside peptides, or instead of them.
Some do, with strong evidence — especially the GLP-1 agonists and the dual agonists. Studies show roughly 15–22% body-weight reduction alongside lifestyle changes. But effectiveness varies between individuals, and results depend on supervision, dosing, and commitment to diet and exercise.
On current evidence, tirzepatide (GLP-1/GIP) appears most effective, with studies showing up to roughly 22.5% weight reduction. Semaglutide follows at 15–20%. "Best," though, is relative to individual factors — medical history, side-effect tolerance, budget, and goals.
Safety varies dramatically by type, and depends on supervision. FDA-approved GLP-1 agonists have known safety profiles from extensive testing. Research compounds carry more risk, from limited data and variable quality. Only a licensed provider can determine safety for a specific situation.
Most show first effects within 2–8 weeks. GLP-1 agonists often reduce appetite within the first week, with measurable loss after 4–6 weeks and maximum benefit after 3–6 months. AOD-9604 and other lipolytic peptides tend to work more gradually.
Some clinicians combine them. But peptide combinations should only be used under close medical supervision, because of possible interactions and compounded side effects. Never self-prescribe combinations.
GLP-1 agonists (semaglutide, liraglutide, tirzepatide) for appetite and blood-sugar control. Dual and triple agonists (tirzepatide, retatrutide) for multi-pathway effects. AOD-9604 for targeted lipolysis. Mitochondrial peptides (MOTS-c, SS-31) for metabolic support. And the GH secretagogues (CJC-1295, ipamorelin, tesamorelin) for hormonal support.
No peptide targets only belly fat — spot reduction isn't physiologically possible. But several reduce visceral abdominal fat. GLP-1 and dual agonists greatly reduce visceral fat in trials. Tesamorelin is FDA-approved for abdominal fat in HIV patients. AOD-9604 was designed to target stubborn deposits, though with limited human data.
AOD-9604 is a modified fragment of human growth hormone (amino acids 177-191), engineered to keep HGH's fat-mobilizing properties while removing growth promotion. Research suggests it may boost lipolysis and block lipogenesis, but human data is limited and it isn't FDA-approved for weight loss.
Explore PrymaLab's research hub and its peptides & weight loss guide for the deeper research on each compound.
Browse Peptide Guides →